A0 - Please enter respondent unique id
Section A: Introduction and screening
This research is being conducted by an independent market research company called Insight Dojo and is on the topic of
Opioid Induced Constipation
We are really interested to hear about your experiences in the area, and your responses will help shape the products and services that are available to people such as yourself.
Some of the questions in this survey are of a sensitive nature, but please be assured that any information you provide us with today will remain fully confidential, and none of the responses will be attributed to you personally.
In the first section we would like to ask a few basic questions about your health and medication. This section will take approximately 5 minutes to complete, but all questions must be filled in in order to progress.
Q1 - What is your gender?
Q2 - How old are you?
Q3 - Thinking specifically about your health, which of the following, if any, apply:
Q4a - Thinking about the pain for which you are currently taking medication, which of the following best describes this:
Q4b - You mentioned that you are currently taking medication to control pain. For which of these following conditions are you currently taking medication to control?
Q5 - Which of these pain conditions causes you the most severe pain i.e., the one for which you need the strongest pain treatment?
Q6
-
Given below is a list of opioid drugs that people take for pain relief.
Are you currently taking any from the list below:
dOpiods - dOpiods (Auto Select)
Q6b - Which of the following formats of opioid medication are you currently taking for pain relief?
Q7 - Roughly, how long ago were you first prescribed opioid drugs for {{Q5}}?
Now we would like to ask you a few questions about your digestive health e.g., pain or discomfort related to your stomach or bowels. Let us start with your bowel movements.
Q8a - Over the past ONE week, on how many days did you have bowel movements?
Q8b - To what extent is moving your bowels bothersome for you (e.g. because you cannot use the toilet as often as you would like, or because you experience pain, discomfort, or difficulties with daily activities)?
Q10
-
Thinking back to the time before you started taking opioid medications.
How was your experience of constipation then compared to the constipation you have now?
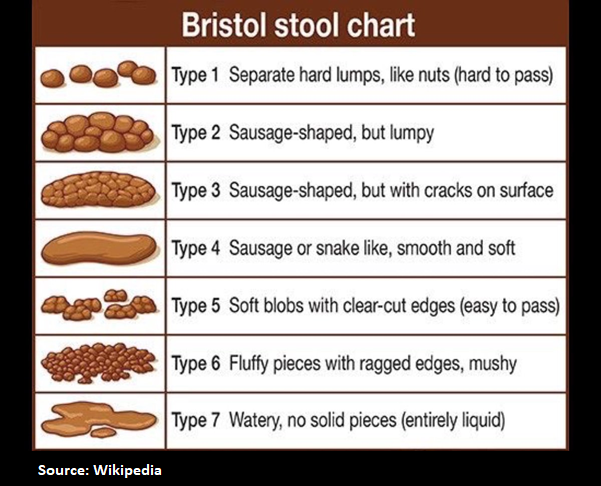
Q10b
-
Below is a chart that represents different types of stools.
Which of the stool types shown on the chart have you experienced in the past week? Select all that apply.